
Page 15 - Rosemead Fall 2025
P. 15
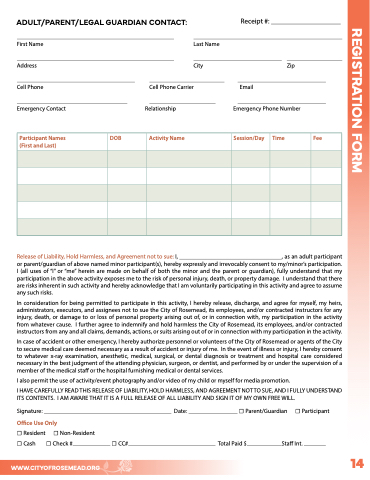
ADULT/PARENT/LEGAL GUARDIAN CONTACT: Receipt #:
First Name Last Name
Address City Zip
Cell Phone Cell Phone Carrier Email
Emergency Contact Relationship Emergency Phone Number
Participant Names
(First and Last)
DOB Activity Name Session/Day Time Fee
REGISTRATION FORM
Release of Liability, Hold Harmless, and Agreement not to sue: I, , as an adult participant
or parent/guardian of above named minor participant(s), hereby expressly and irrevocably consent to my/minor’s participation.
I (all uses of “I” or “me” herein are made on behalf of both the minor and the parent or guardian), fully understand that my
participation in the above activity exposes me to the risk of personal injury, death, or property damage. I understand that there
are risks inherent in such activity and hereby acknowledge that I am voluntarily participating in this activity and agree to assume
any such risks.
In consideration for being permitted to participate in this activity, I hereby release, discharge, and agree for myself, my heirs,
administrators, executors, and assignees not to sue the City of Rosemead, its employees, and/or contracted instructors for any
injury, death, or damage to or loss of personal property arising out of, or in connection with, my participation in the activity
from whatever cause. I further agree to indemnify and hold harmless the City of Rosemead, its employees, and/or contracted
instructors from any and all claims, demands, actions, or suits arising out of or in connection with my participation in the activity.
In case of accident or other emergency, I hereby authorize personnel or volunteers of the City of Rosemead or agents of the City
to secure medical care deemed necessary as a result of accident or injury of me. In the event of illness or injury, I hereby consent
to whatever x-ray examination, anesthetic, medical, surgical, or dental diagnosis or treatment and hospital care considered
necessary in the best judgment of the attending physician, surgeon, or dentist, and performed by or under the supervision of a
member of the medical staff or the hospital furnishing medical or dental services.
I also permit the use of activity/event photography and/or video of my child or myself for media promotion.
I HAVE CAREFULLY READ THIS RELEASE OF LIABILITY, HOLD HARMLESS, AND AGREEMENT NOT TO SUE, AND I FULLY UNDERSTAND
ITS CONTENTS. I AM AWARE THAT IT IS A FULL RELEASE OF ALL LIABILITY AND SIGN IT OF MY OWN FREE WILL.
Signature: Date: ☐ Parent/Guardian ☐ Participant
Office Use Only
☐ Resident ☐ Non-Resident
☐ Cash ☐ Check # ☐ CC# Total Paid $ Staff Int.
14
WWW.CITYOFROSEMEAD.ORG
